Mark Grzeskowiak, RCP, RRT, FAARC
 In January 2006, President Bush signed the Deficit Reduction Act, which created a system for reducing Medicare payments to hospitals whose patients develop higher rates of hospital-acquired conditions. In March 2010, the Patient Protection and Affordable Care Act was signed into law and among its many goals is the improvement of the quality and efficiency of health care through the use of financial incentives. Protecting patients from harm has always been the right thing to do, but in health care’s current pay-for-performance era, the concept of patient safety has taken on new emphasis. Although it is not directly related to either of the above-mentioned programs, another change relating to safety and quality of care will take place in January 2013. This one unquestionably impacts the role of the respiratory care practitioner and the way care is provided for ventilator patients.
In January 2006, President Bush signed the Deficit Reduction Act, which created a system for reducing Medicare payments to hospitals whose patients develop higher rates of hospital-acquired conditions. In March 2010, the Patient Protection and Affordable Care Act was signed into law and among its many goals is the improvement of the quality and efficiency of health care through the use of financial incentives. Protecting patients from harm has always been the right thing to do, but in health care’s current pay-for-performance era, the concept of patient safety has taken on new emphasis. Although it is not directly related to either of the above-mentioned programs, another change relating to safety and quality of care will take place in January 2013. This one unquestionably impacts the role of the respiratory care practitioner and the way care is provided for ventilator patients.
The newest challenge will focus on mitigating the development of ventilator-associated pneumonia (VAP). VAP is now recognized as one of the most common and most frequently fatal type of hospital-acquired infection. Published data show that VAP accounts for more deaths than urinary tract infections, infections from central lines, or surgical site infections.1
In an effort to raise awareness and lessen its rise, a collection of practices that became known as a ventilator bundle was proposed in 1999. Since that time, other groups developed their own bundles,2-4 and although the elements varied, their goal was essentially the same.
Since the first version of the vent bundle was brought into practice, it is fair to say that it has had a positive effect. The literature is full of case reports and studies that describe how rates for VAP have dropped as a result of its use. In an effort to spread the message, the Institute for Healthcare Improvement (IHI) established a group referred to as “mentor hospitals,” which have described their efforts to control and, in some cases, eliminate this problem.
If there is an intention to reward those who do a good job of preventing hospital-acquired infections, the objective basis for VAP diagnosis should be sound. Unfortunately, it is not. As an example, the current criteria attempt to quantify VAP with an evaluation of the patient’s sputum. Changes in consistency, color, or quantity were felt to be indicative of a pneumonic process. Unfortunately, these terms are far too subjective to be of any real scientific value. A change in a patient’s chest x-ray is another confirmatory indicator. The presence of a new or persistent infiltrate is considered to be a sign of impending compromise. But the variability in both radiographic technique and the opinions of interpreting radiologists makes this an equally unreliable indicator. In their Ventilator-Associated Event Protocol, the National Health and Safety Network describes the currently used criteria as “neither sensitive nor specific.” If this statement is correct, a number of questions occur. If you cannot reliably confirm VAP, how do you know what your rates really are? Also, how would you know if a prevention strategy is working?
In an effort to eliminate the subjectivity of the VAP diagnostic criteria, the Centers for Disease Control and Prevention (CDC) convened a group of health care experts to discuss how the process could be improved. The group met for the first time in 2011 and included representatives from the American Society of Critical-Care Nurses, National Institutes of Health, American Association for Respiratory Care, American Thoracic Society, American College of Chest Physicians, Society of Critical Care Medicine, Council of State and Territorial Epidemiologists, HICPAC surveillance working group, US Department of Health and Human Services, Infectious Diseases Society of America, Society for Healthcare Epidemiology of America, and Association for Professionals in Infection Control and Epidemiology.
One of the first tasks undertaken was to identify a wide variety of ventilator-associated conditions and an objective basis for determining when they existed. VAP will no longer be the only condition being evaluated. The result of their work was a new algorithm that will include definitions for three potentially preventable events that could develop in ventilator patients. Those tiers include 1) ventilator-associated conditions (VAC), 2) infection-related ventilator-associated conditions (IVAC), and 3) possible or probable VAP. One should anticipate seeing the changes in terminology described below.
Ventilator-Associated Events (VAE)
Ventilator-Associated Conditions (VAC)
Infection-Related Ventilator-Associated Conditions (IVAC)
Probable/Possible Ventilator-Associated Pneumonia (VAP)
Ventilator-Associated Event (VAE) Algorithm
The algorithm will be applied only to patients who are 18 years or older and are being cared for at acute care facilities, long-term care facilities, and inpatient rehabilitation facilities.
The CDC states that the algorithm is used for surveillance purposes only and is not intended to guide the clinical management of patients. The guidelines in their entirety can be found at www.cdc.gov and searching for “ventilator-associated event protocol.”

Figure 1 (click to enlarge) attempts to provide a general overview of how VAEs will be classified in the months to come. The conditions IVAC and VAC were designed for potential use in public-reporting, pay-for–performance programs or even interfacility comparisons. A more detailed explanation of each event type appears in the following paragraphs.
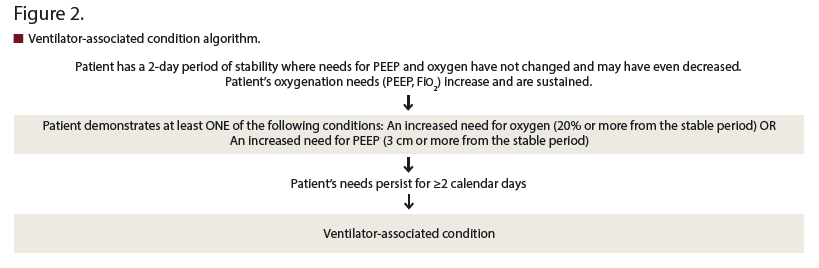
Ventilator-Associated Condition (VAC) Algorithm
The usual course for a patient placed on mechanical support involves an initial period of fluctuating ventilatory needs, but at some point they should achieve a period of stabilization where their needs for PEEP and supplemental oxygen plateau or even decrease. If patients attain a stable period and remain there for at least 2 days, but then their needs for oxygen increase by 20% or more, or their needs for PEEP increase by 3 cm or more, and these needs are sustained for 2 days or more, those who conduct surveillance should record this as a VAC (Figure 2; click to enlarge).
The patient shown in Figure 3 (click to enlarge) developed a VAC because their need for oxygen increased by 20% over the baseline period of stability reached on day 4.

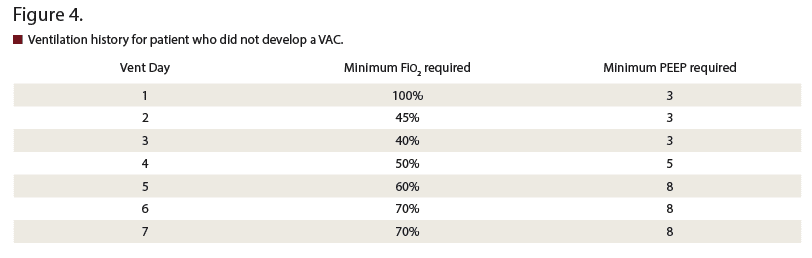
The patient shown in Figure 4 (click to enlarge) did not develop a VAC because they never achieved a 2-day period of stability with regard to their need for oxygen and/or PEEP.
Important Points Regarding VAC.
• The patient’s needs for oxygen must attain a level of stability. If they are started on an FiO2 of 50%, but their needs continue to increase before ultimately expiring, they could not have developed a VAC because they never attained a stable state.
• The earliest a VAC can occur is day 4. This is because a patient must have at least 2 days of oxygenation stability. This must be followed by at least 2 days of increased needs for PEEP or FiO2.
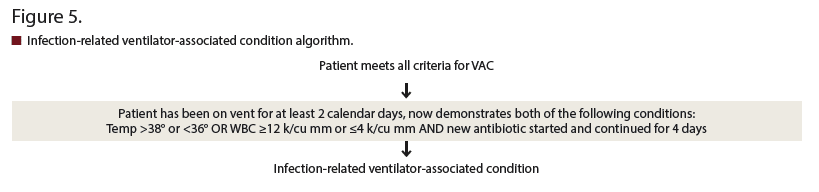
Infection-Related Ventilator-Associated Condition (IVAC) Algorithm
Patients who develop a VAC also may experience a period where they develop an infective or inflammatory process. The severity of this phase can be evaluated with the tier shown in Figure 5 (click to enlarge).
Important Points Regarding IVAC.
• If a patient satisfies the criteria for VAC, they may also satisfy the criteria for an IVAC.
• It is possible that patients can have elevated white blood cell counts and have a new antibiotic started, but unless they also meet the criteria for VAC, VAE should not be recorded.
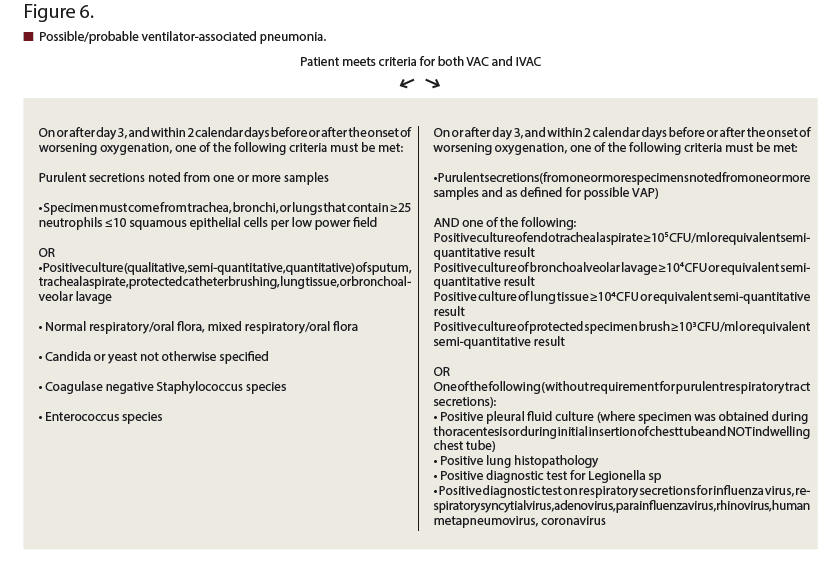
The Possible/Probable VAP algorithm in Figure 6 (click to enlarge) was developed so that hospitals might use it for internal quality improvement projects.
Ventilator Patients: Who’s In, Who’s Out? The CDC’s new program has specific criteria regarding its application to ventilator patients. Positive pressure ventilators (IPPB, CPAP, BiPAP) are not considered “ventilators” in this context unless they are attached to a patient’s endotracheal or tracheostomy tube.
Patients who are ventilated with APRV or a related mode (PCV+, Bilevel, Bi vent, BiPhasic, Duo PAP) should be included in surveillance, but only changes in their FiO2 requirement can be used to determine a qualifying deterioration in their oxygenation status.
Also included are patients being ventilated with conventional mode but are in the prone position or receiving pulmonary vasodilator therapy (epoprostenol, inhaled nitric oxide).
Patients should be excluded from surveillance if they are:
• Under the age of 18
• Being ventilated with high frequency ventilation or
• Receiving extracorporeal membrane oxygen therapy (ECMO)
Patients who are extubated for at least one calendar day but then require reintubation begin a new period of mechanical ventilation.
Miscellaneous Points Regarding Surveillance. Currently, there are no federal requirements to report VAEs, and at this time it is not a reportable event, according to the CMS Hospital Inpatient Quality Reporting program. However, this is subject to changes implemented at the federal or state level.
Preventative Measures
Many hospitals have implemented some form of ventilator bundle, but it is clear that the changes described above could easily translate into many more potentially reportable cases. Continuing to follow the basic elements of the ventilator bundle may not be enough. In the spirit of being proactive, instead of reactive, respiratory care practitioners are encouraged to review some of the strategies described below. Implementing some or all may be helpful in lessening the number of VAEs.
Suctioning Practices. The removal of tracheal secretions from a patient’s artificial airway is a routine practice, but preventing ventilator-associated events will likely require some modification. Caregivers need to consider the secretions in the patient’s mouth and those trapped at the level of the cuff of the airway. These secretions can be more effectively cleared through the use of airways with suction ports above the cuff. A less expensive option would be to use suction catheters specifically designed to reach these areas.
Another method that may be helpful in removing these secretions was reported many years ago by Jamil.5 He describes a way of using positive pressure to push secretions from the top of the cuff in a cephalad direction so they can be more easily cleared. Although the actual process varies, the same concept has been reported by others.6,7
Minimize Circuit Breaks. Dave et al demonstrated that positive pressure was helpful in minimizing the transfer of accumulated secretions from above the cuff.8 Each time the patient is disconnected from their circuit, there will be a decrease in intrathoracic pressure, which could allow for a mini-aspiration event.
Prevent Aspiration During Transport. In an article published in 1997, Kollef et al reviewed a number of factors that they felt could contribute to the likelihood of patients developing VAP. They calculated that the odds ratio in patients who underwent transport was nearly four times greater than in those patients who were not transported.9 Movement of the patient from bed to gurney and then from gurney to exam table produces a lot of back and forth endotracheal tube movement as well. It is possible that keeping the patient supine also could contribute to aspiration. A practice that requires more aggressive suctioning could be helpful. This would include suctioning the patient’s mouth and above the cuff of the patient’s artificial airway. To be thorough, the patient should be suctioned prior to leaving their room, after the procedure is finished, and again after the patient returns to their room.
Minimizing ventilator days through an efficiently run weaning protocol is the key to decreasing the incidence of ventilator-associated sequelae. But planning for the unanticipated should be a part of every ICU patient’s plan of care. VAP has always been a multifactorial problem, and thus, its resolution will require a similarly structured plan.
In addition to the algorithms described above, the CDC website provides copies of several forms and highly detailed instructions on how the surveillance process should be conducted. It should be anticipated that processing this information and putting it into practice will take some time and effort (the document on the web page is 53 pages long). It will not be easy to understand and implement for those who monitor quality improvement and hospital-acquired infections. Representatives from those groups are almost certain to need help interpreting ventilator records to determine if or when PEEP or FiO2 changes have been made or if those changes meet the threshold of significance. It is also unlikely that they understand the concept of bilevel ventilation or APRV. But working through the learning process could provide a perfect opportunity for respiratory care departments to collaborate with them and demonstrate another aspect of the value of respiratory care.
Mark Grzeskowiak, RCP, RRT, FAARC, is manager, education and quality, Respiratory Care Services, Long Beach Memorial Medical Center, Long Beach, Calif. For further information, contact [email protected].
REFERENCES
1. Klevens RM, Edwards JR, Richards CL Jr, et al. Estimating health care-associated infections and deaths in U.S. hospitals, 2002. Public Health Rep. 2007;122:160-166.
2. Torres A, Carlet J. Ventilator-associated pneumonia. European Task Force on Ventilator-Associated Pneumonia. Eur Respir J. 2001;17:1034–1045.
3. Dodek P, Keenan S, Cook D, et al; Canadian Critical Care Trials Group, Canadian Critical Care Society. Evidence-based clinical practice guideline for the prevention of ventilator-associated pneumonia. Ann Intern Med. 2004;141:305–313.
4. American Thoracic Society (ATS) and Infectious Diseases Society of America (IDSA). Guidelines for the management of adults with hospital acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388–416.
5. Jamil AK. Laryngeal toilet before extubation. Anaesthesia. 1974;29(5):630-631.
6. Miller KA, Harkin CP, Bailey PL. Postoperative tracheal extubation. Anesth Analg. 1995;80(1):149-172.
7. Cole LB, Hase R, Bard J. Clearing secretions from above the endotracheal tube cuff using a purge maneuver: a bench study [abstract]. Resp Care. 2008;55(11):1517.
8. Dave MH, Koepfer N, Madjdpour C, Frotzier A, Weiss M. Tracheal fluid leakage in benchtop trials: comparison of static v. dynamic ventilation model with and without lubrication. J Anesth. 2010;24(2):247-52
9. Kollef M, Von Harz B, Prentice D, et al. Patient transport from intensive care increases the risk for ventilator-associated pneumonia. Chest. 1997;112(3):765-73.








