Pulmonary function testing allows a physician to realize the extent of a patient’s asthmatic compromise
This study will report on a 38-year-old Hispanic woman who has been a patient of the Providence Community Health Centers since 1983. We will refer to her by the pseudonym Mary.
Mary is a wonderful example of the importance of using pulmonary function testing (PFT) for better assessment and care for individuals with respiratory concerns.
Mary first presented with shortness of breath (SOB) in 1995. At the time, she was prescribed an albuterol inhaler as needed. From 1995 through the present, Mary appears to have been a responsible patient, presenting for routine examinations as well as sporadic sick visits. During these 10 years, Mary occasionally complained of SOB, chest tightness, cough, and, at times, increased pulmonary mucus. There were frequently long periods of time between complaints, and there was no easy-to-discern pattern to these complaints. Several times over this period, Mary received additional albuterol inhalers. Only once in 2003 was a physician able to hear any wheezing.
In September 2005, Mary presented to her primary care physician (PCP) with SOB, coughing, and complaints of cold-like symptoms. Her physician did not hear wheezing at that time and wanted to examine further what might be at the root of Mary’s discomfort.
On October 3, 2005, Mary presented to the certified asthma educator for spirometry. Prior to testing, Mary stated that she was feeling very well that day and that she did not expect the test to reveal anything abnormal. She said that she had been uncomfortable the week before and had been using the albuterol multiple times per day. On this day, however, she reported that she was fine and felt completely normal.
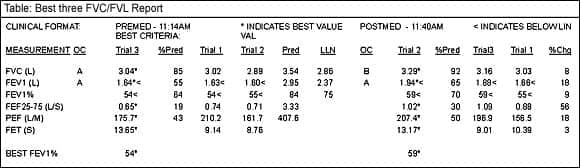
Her tests at this time revealed severely obstructed airways (See Table). Her FVC was 85% of her predicted normal values based on her age, height, gender, and ethnicity. Her FEV1 was 55% of her predicted normal values, her FEV1/FVC (FEV1%) was only 54%, and her FEF25-75 was 19% of predicted. Albuterol via nebulizer was administered at this time, and she responded with a significant improvement. Her FEV1 increased 18% and her FEF25-75 increased 56% post-bronchodilator therapy. Mary did admit that she felt much better and had not realized that she was tight or compromised, but now she realized that her condition had improved.
The spirometry allowed Mary’s physician to realize the extent of her asthmatic compromise, and Mary was prescribed medications to control the inflammation associated with her asthma. The certified asthma educator taught Mary how to properly use this medication and the importance of participating in daily asthma management. Other information about the disease of asthma was discussed, including normal versus asthmatic airways and controller versus rescue medication. Mary returned 3 weeks later for peak flow meter education and asthma diary development. Mary also followed up with her PCP and reported a very significant improvement in her comfort. She reported that she did not use albuterol at all for 6 weeks and was very happy with her current plan. The physician wondered if it would be possible to reduce Mary’s controller medications at this time.
To help answer this question, on December 5, 2005, the certified asthma educator performed another spirometry test with Mary. This test showed a tremendous improvement compared to her initial examination, although mild compromise was still noted. At this second examination, her FVC was 98% of predicted, an increase of 14%; FEV1 was 77% of predicted, an increase of 40%; FEV1% was 66%, an increase of 22%; and FEF25-75 was 40% of predicted, an increase of 108%. While the subjective and objective data both revealed a big improvement, the objective data was able to show that the patient continued to have some compromise and that it would not be prudent to reduce the medications at this time.
The patient was further complimented and educated throughout this process, and her responsible use of her medications was strongly reinforced. Mary is scheduled to return to the asthma educator in 2 months for continued education and evaluation.

Eliza Beringhause, MEd, RRT, AE-C, is an asthma educator, Providence Community Health Center, Providence, RI.








